Module 1 Slides - no narration (1)Open original source page
Original source file is included in this package; the embedded viewer and full extracted text are available below.
Slide Text Extract
Improved reading view: slide text is enlarged, spaced out, and placed in expandable study cards. Use Expand all to read continuously, or search the whole textbook from the search box.
Images embedded in the deck are shown after the slide text. Open the original PPTX for exact slide layout.
Slide 1
Pharmacotherapeutics for Advanced Practice:
Module 1
N609
N609
Slide 2
Part 1
Issues for the Practitioner in Drug Therapy
Slide 3
Learning Objectives
Describe the approval process for prescribed drugs in the United States.
Analyze the practitioner's role and responsibilities in prescribing.
Explain the process for prescribing, whether in writing or through the electronic health record.
Analyze the practitioner's role and responsibilities in prescribing.
Explain the process for prescribing, whether in writing or through the electronic health record.
Slide 4
Drug Safety and Market Safeguards
Role of the U.S. Food and Drug Administration (FDA)
Conducting and monitoring clinical trials
Approving new drugs for market and manufacture
Ensuring safe drugs for public consumption
Conducting and monitoring clinical trials
Approving new drugs for market and manufacture
Ensuring safe drugs for public consumption
Slide 5
Clinical Trials
Slide 6
Question #1
It has been determined by the FDA that a new drug causes no apparent serious adverse effects and the dosage range is appropriate. Double-blind studies are planned to compare the drug to a placebo. This drug is in what phase of clinical trials?
A. Phase I
B. Phase II
C. Phase III
D. Phase IV
A. Phase I
B. Phase II
C. Phase III
D. Phase IV
Slide 7
Answer to Question #1
C. Phase III
Rationale: In Phase III, double-blind research methods are used for data collection, and the drug is compared with a placebo. In Phase I, an initial evaluation of the drug is conducted. In Phase II, drug effects are monitored on up to several hundred patients who have the disease. Postmarketing surveillance occurs in Phase IV.
Rationale: In Phase III, double-blind research methods are used for data collection, and the drug is compared with a placebo. In Phase I, an initial evaluation of the drug is conducted. In Phase II, drug effects are monitored on up to several hundred patients who have the disease. Postmarketing surveillance occurs in Phase IV.
Slide 8
FDA Fast Track
Four categories for which pharmaceutical companies request review
Fast track
Breakthrough therapy
Accelerated approval
Priority review
Fast track
Breakthrough therapy
Accelerated approval
Priority review
Slide 9
Prevention of Harm and Misuse
Five categories of scheduled drugs:
Schedule 1: high potential for abuse; no routine therapeutic use
Schedule 2: valid medical use; high potential for abuse
Schedule 3: Potential for abuse is lower than drugs on Schedule 2; prescriptions cannot be refilled.
Schedule 4: low potential for abuse; limited physiologic dependency
Schedule 5: least potential for abuse; moderate amount of opioids
Schedule 1: high potential for abuse; no routine therapeutic use
Schedule 2: valid medical use; high potential for abuse
Schedule 3: Potential for abuse is lower than drugs on Schedule 2; prescriptions cannot be refilled.
Schedule 4: low potential for abuse; limited physiologic dependency
Schedule 5: least potential for abuse; moderate amount of opioids
Slide 10
Question #2
A practitioner prescribes codeine for a patient who is postoperative following knee surgery. What schedule drug is being prescribed?
A. Schedule 1
B. Schedule 2
C. Schedule 3
D. Schedule 4
E. Schedule 5
A. Schedule 1
B. Schedule 2
C. Schedule 3
D. Schedule 4
E. Schedule 5
Slide 11
Answer to Question #2
C. Schedule 3
Rationale: Examples of Schedule 3 drugs are certain narcotics such as codeine and nonbarbiturate sedatives. Examples of Schedule 1 drugs are heroin and lysergic acid diethylamide. Examples of Schedule 2 drugs are certain amphetamines and barbiturates. Examples of Schedule 4 drugs are nonnarcotic analgesics and antianxiety agents. Examples of Schedule 5 drugs include antitussives and antidiarrheals containing small amounts of narcotics.
Rationale: Examples of Schedule 3 drugs are certain narcotics such as codeine and nonbarbiturate sedatives. Examples of Schedule 1 drugs are heroin and lysergic acid diethylamide. Examples of Schedule 2 drugs are certain amphetamines and barbiturates. Examples of Schedule 4 drugs are nonnarcotic analgesics and antianxiety agents. Examples of Schedule 5 drugs include antitussives and antidiarrheals containing small amounts of narcotics.
Slide 12
Practitioner's Role and Responsibilities in Prescribing
Drug selection
Concerns related to ethics and practice
Patient education
Prescriptive authority
Drug sampling
Concerns related to ethics and practice
Patient education
Prescriptive authority
Drug sampling
Slide 13
Steps of the Prescribing Medications
Slide 14
National Provider Identifier (NPI)
Identify all health care providers by a unique number in standard transactions (e.g., health care claims).
Identify health care providers on prescriptions.
Link provider ID numbers in internal files.
Coordinate benefits between health plans.
Update patient medical-record systems.
Use in program integrity files.
Identify health care providers on prescriptions.
Link provider ID numbers in internal files.
Coordinate benefits between health plans.
Update patient medical-record systems.
Use in program integrity files.
Slide 15
Steps of the Prescribing Medications
Selecting the most appropriate agent
Considerations of special populations
Identifying outcomes
Considerations of special populations
Identifying outcomes
Slide 16
Writing the Prescriptions
Date, name, address, and date of birth
Prescriber's name, address, and phone number
Name of drug
Dose, dosage regimen, and route of administration
Allowable substitutions
Prescriber's signature and license number
Prescriber's name, address, and phone number
Name of drug
Dose, dosage regimen, and route of administration
Allowable substitutions
Prescriber's signature and license number
Slide 17
Question #3
A health care provider performs a physical examination of a patient who presents with high blood pressure. When choosing a hypertensive for the patient, what step in the prescribing process follows the formulation of the diagnosis of hypertension?
A. Review the pathophysiology of the disease.
B. Select the most appropriate agent.
C. Evaluate the patient's response to the therapy.
D. Consider second-line therapy for the patient.
A. Review the pathophysiology of the disease.
B. Select the most appropriate agent.
C. Evaluate the patient's response to the therapy.
D. Consider second-line therapy for the patient.
Slide 18
Answer to Question #3
A. Review the pathophysiology of the disease.
Rationale: The order of the process for prescribing a drug is assess, diagnose, review pathophysiology of disease, select a first-line therapy, evaluate patient response, maintain regimen or move to second-line therapy, reevaluate, maintain regimen, or move to third-line therapy.
Rationale: The order of the process for prescribing a drug is assess, diagnose, review pathophysiology of disease, select a first-line therapy, evaluate patient response, maintain regimen or move to second-line therapy, reevaluate, maintain regimen, or move to third-line therapy.
Slide 19
Electronic Prescriptions
Improved legibility of prescriptions and rate of completed prescriptions
Greater patient convenience at pharmacy
Increased compliance with formulary requirements
Decreased drug-drug interactions
Reduced medication errors with use of drug-checking software
Greater patient convenience at pharmacy
Increased compliance with formulary requirements
Decreased drug-drug interactions
Reduced medication errors with use of drug-checking software
Slide 20
Adherence Issues
Approachability of health care provider
Perception of respect with which they are treated by the practitioner
Belief the therapy is beneficial
Belief the benefits of therapy outweigh the risks or side effects
Degree to which the patient participates in developing the treatment regimen
Cost of the regimen
Perception of respect with which they are treated by the practitioner
Belief the therapy is beneficial
Belief the benefits of therapy outweigh the risks or side effects
Degree to which the patient participates in developing the treatment regimen
Cost of the regimen
Slide 21
Adherence Issues
Simplicity and understanding of the regime
Degree to which the patient feels that expectations are being met
Degree to which the patient perceives their concerns are important and being addressed
Degree to which the practitioner motivates the patient to adhere to the regimen
Degree to which the regimen is compatible with the patient's lifestyle
Degree to which the patient feels that expectations are being met
Degree to which the patient perceives their concerns are important and being addressed
Degree to which the practitioner motivates the patient to adhere to the regimen
Degree to which the regimen is compatible with the patient's lifestyle
Slide 22
Adverse Drug Events
Lack of drug knowledge
Lack of patient information
Poor communication
Special population considerations
Lack of patient information
Poor communication
Special population considerations
Slide 23
Pharmacogenomics
Many different genes influence the way a person responds to a drug.
Without knowing all the genes involved in drug response, it has not been possible to develop genetic tests that could predict a person's response to a drug.
Without knowing all the genes involved in drug response, it has not been possible to develop genetic tests that could predict a person's response to a drug.
Slide 24
Updating Drug Information
Reference books
Pharmacists
Easy-to-carry drug handbooks
Pocket guides
Pharmacists
Easy-to-carry drug handbooks
Pocket guides
Slide 25
Summary
Drug therapy is often the mainstay of acute and chronic diseases, and in many cases, health care practitioners include it in the patient treatment plan.
Many issues require consideration when planning drug therapy, including product safeguards, writing the prescription, patient adherence, follow-up measures, and keeping up-to-date with new developments.
It is imperative that prescribers have the best knowledge of the principles of prescribing to prevent errors and develop safe, appropriate, and effective drug therapy.
Many issues require consideration when planning drug therapy, including product safeguards, writing the prescription, patient adherence, follow-up measures, and keeping up-to-date with new developments.
It is imperative that prescribers have the best knowledge of the principles of prescribing to prevent errors and develop safe, appropriate, and effective drug therapy.
Slide 26
Part 2
Pharmacokinetic Basis of Therapeutics and Pharmacodynamic Principles
Slide 27
Learning Objectives
Describe the difference between pharmacokinetics and pharmacodynamics.
Discuss the impact of each of the four pharmacokinetic principles on medications administered to a patient: absorption, distribution, metabolism, and elimination.
Describe the concept of affinity and differentiate between an antagonist and an agonist.
Apply the knowledge of pharmacokinetic principles to considerations of a patient case scenario.
Given patient details, calculate renal function utilizing the Cockcroft-Gault formula and the Modification of Diet in Renal Disease (MDRD) equation.
Discuss the impact of each of the four pharmacokinetic principles on medications administered to a patient: absorption, distribution, metabolism, and elimination.
Describe the concept of affinity and differentiate between an antagonist and an agonist.
Apply the knowledge of pharmacokinetic principles to considerations of a patient case scenario.
Given patient details, calculate renal function utilizing the Cockcroft-Gault formula and the Modification of Diet in Renal Disease (MDRD) equation.
Slide 28
Pharmacokinetics versus Pharmacodynamics
Pharmacokinetics
Refers to the movement of the drug through the body and how the body affects the drug.
Drug administration, absorption, distribution, and elimination are involved.
Pharmacodynamics
Refers to how the drug affects the body; how the drug initiates its therapeutic or toxic effect at the cellular level and systemically.
Refers to the movement of the drug through the body and how the body affects the drug.
Drug administration, absorption, distribution, and elimination are involved.
Pharmacodynamics
Refers to how the drug affects the body; how the drug initiates its therapeutic or toxic effect at the cellular level and systemically.
Slide 29
Relationship Between Pharmacokinetics and Pharmacodynamics
Slide 30
Pharmacokinetics
Factors affecting absorption
Movement through membranes and drug solubility
Passive diffusion
Active transport
Pharmaceutical preparation
Blood flow
Gastrointestinal motility
Enteral absorption
Oral administration
Sublingual administration
Rectal administration
Parenteral absorption
Inhalation
Intravenous administration
Subcutaneous administration
Intramuscular administration
Topical administration
Transdermal administration
Movement through membranes and drug solubility
Passive diffusion
Active transport
Pharmaceutical preparation
Blood flow
Gastrointestinal motility
Enteral absorption
Oral administration
Sublingual administration
Rectal administration
Parenteral absorption
Inhalation
Intravenous administration
Subcutaneous administration
Intramuscular administration
Topical administration
Transdermal administration
Slide 31
Question #1
A patient is given a medication for hypertension that is absorbed enterally. Via what route might this medication be administered?
A. Intramuscular
B. Subcutaneous
C. Oral
D. Topical
A. Intramuscular
B. Subcutaneous
C. Oral
D. Topical
Slide 32
Answer to Question #1
C. Oral
Rationale: Enteral absorption occurs after a drug is administered by the oral or rectal route. Parenteral absorption is associated with drugs administered intramuscularly, subcutaneously, or topically.
Rationale: Enteral absorption occurs after a drug is administered by the oral or rectal route. Parenteral absorption is associated with drugs administered intramuscularly, subcutaneously, or topically.
Slide 33
Question #2
A health care practitioner orders a loading dose of an antibiotic for a patient with bacteremia. What would be the preferred route to ensure maximum bioavailability?
A. Oral
B. Subcutaneous
C. Intramuscular
D. Intravenous
A. Oral
B. Subcutaneous
C. Intramuscular
D. Intravenous
Slide 34
Answer to Question #2
D. Intravenous
Rationale: The intravenous route provides rapid access to the circulatory system with a known quantity of drug; the IV route of administration assures 100% bioavailability, thus it is considered the gold standard. Absorption after oral administration is slow and depends on the patient's gastric emptying time. Subcutaneous administration produces a slower, more prolonged release of medication into the bloodstream. A wide variability in the rate of absorption results from injections given intramuscularly due to use in different muscles and in different patients.
Rationale: The intravenous route provides rapid access to the circulatory system with a known quantity of drug; the IV route of administration assures 100% bioavailability, thus it is considered the gold standard. Absorption after oral administration is slow and depends on the patient's gastric emptying time. Subcutaneous administration produces a slower, more prolonged release of medication into the bloodstream. A wide variability in the rate of absorption results from injections given intramuscularly due to use in different muscles and in different patients.
Slide 35
Distribution
Protein binding
Volume of distribution
Volume of distribution
Slide 36
Plasma Protein Binding
Slide 37
Calculating the Apparent Volume of Distribution (Vd)
Slide 38
Elimination
Metabolism
Drug excretion
Half-life
Steady state
Clearance
Drug excretion
Half-life
Steady state
Clearance
Slide 39
Pharmacodynamics
Drug receptors
A receptor is the component of the cell (or an enzyme) to which an endogenous substance binds, or attaches, initiating a chain of biochemical events.
The capacity of a drug to bind to a receptor depends on the size and shape of the drug and the receptor.
Drug receptors are commonly classified by the effect they produce.
A receptor is the component of the cell (or an enzyme) to which an endogenous substance binds, or attaches, initiating a chain of biochemical events.
The capacity of a drug to bind to a receptor depends on the size and shape of the drug and the receptor.
Drug receptors are commonly classified by the effect they produce.
Slide 40
Four Types of Receptors
Gated ion channels
Transmembranous receptors: cytoplasmic enzyme or tyrosine kinase activated
G protein-coupled receptors
Intracellular receptors
Transmembranous receptors: cytoplasmic enzyme or tyrosine kinase activated
G protein-coupled receptors
Intracellular receptors
Slide 41
Drug-Receptor Interactions
Affinity: degree to which a drug is attracted to a receptor.
Chirality: drugs exist in two forms with mirror-image spatial arrangements called enantiomers or isomers, which affect interaction with receptors.
Agonists: drugs that display a degree of affinity for a receptor and stimulate a response.
Antagonists: drugs that display an affinity and do not elicit a response.
Chirality: drugs exist in two forms with mirror-image spatial arrangements called enantiomers or isomers, which affect interaction with receptors.
Agonists: drugs that display a degree of affinity for a receptor and stimulate a response.
Antagonists: drugs that display an affinity and do not elicit a response.
Slide 42
Dose-Response Relationship
Slide 43
Factors Affecting Pharmacokinetics and Pharmacodynamics
Patient variables
Pathophysiology
Genetics
Age
Sex
Ethnicity
Diet and nutrition
Pathophysiology
Genetics
Age
Sex
Ethnicity
Diet and nutrition
Slide 44
Summary
Medications are prescribed to alleviate symptoms, cure disease, or prevent severe morbidity or mortality.
Underpinning the treatment process is the intricate relationship between the body and the medications.
Practitioners must be aware of the effect of pharmacokinetics (movement of the drug through the body) and pharmacodynamics (how the drug affects the body) when prescribing drug therapy for patients.
Underpinning the treatment process is the intricate relationship between the body and the medications.
Practitioners must be aware of the effect of pharmacokinetics (movement of the drug through the body) and pharmacodynamics (how the drug affects the body) when prescribing drug therapy for patients.
Slide 45
Part 3
Impact of Drug Interactions and Adverse Events on Therapeutics
Slide 46
Four Major Categories of Drug Interactions
Drug-drug interactions
Drug-food interactions
Drug-herb interactions
Drug-disease interactions
Drug-food interactions
Drug-herb interactions
Drug-disease interactions
Slide 47
Pharmacokinetic Factors Affecting Drug Therapy
Absorption
Distribution
Metabolism
Excretion
Distribution
Metabolism
Excretion
Slide 48
Pharmacokinetic Interactions: Absorption
Acidity (pH): one drug may alter the acidity of the gastrointestinal (GI) tract
Adsorption: occurs when one agent binds the other to its surface to form a complex
GI motility and rate of absorption: drugs that affect the GI tract can affect the rate of absorption instead of affecting the amount of drug absorbed
GI flora and absorption: bacteria present in the GI tract are responsible for a portion of the metabolism of some agents
Adsorption: occurs when one agent binds the other to its surface to form a complex
GI motility and rate of absorption: drugs that affect the GI tract can affect the rate of absorption instead of affecting the amount of drug absorbed
GI flora and absorption: bacteria present in the GI tract are responsible for a portion of the metabolism of some agents
Slide 49
Distribution of Drugs in Bloodstream
Most are bound to plasma proteins such as albumin or 1-acid glycoprotein.
Only an unbound drug is free to interact with its target receptor site and is therefore active.
The percentage of drug that binds to plasma proteins depends on the affinity of that drug for the protein-binding site.
Clinically significant drug displacement interactions normally occur only when drugs are more than 90% protein bound and have a narrow therapeutic index.
Only an unbound drug is free to interact with its target receptor site and is therefore active.
The percentage of drug that binds to plasma proteins depends on the affinity of that drug for the protein-binding site.
Clinically significant drug displacement interactions normally occur only when drugs are more than 90% protein bound and have a narrow therapeutic index.
Slide 50
Metabolism
Main sites of metabolism
Liver (hepatocytes)
Small intestine (enterocytes)
Kidneys, lungs, brain play minor role
Classification of cytochrome P-450 isoenzymes
Family (>36% homology in amino acid sequence)
Subfamily (77% homology)
Individual gene
Liver (hepatocytes)
Small intestine (enterocytes)
Kidneys, lungs, brain play minor role
Classification of cytochrome P-450 isoenzymes
Family (>36% homology in amino acid sequence)
Subfamily (77% homology)
Individual gene
Slide 51
Inhibition of Drug Metabolism
Affinity: the greater the affinity of an inhibiting drug for an enzyme, the more it blocks binding of other drug molecules
Half-life: determines duration of the interaction
Concentration: threshold concentration must be reached or exceeded to inhibit an enzyme
Toxic potential of the object drug
Efficacy: effectiveness of the object drug
Half-life: determines duration of the interaction
Concentration: threshold concentration must be reached or exceeded to inhibit an enzyme
Toxic potential of the object drug
Efficacy: effectiveness of the object drug
Slide 52
Question #1
A practitioner is prescribing amiodarone for a patient with cardiac arrhythmia. Which factor affecting the duration of the drug must a practitioner consider if an adverse interaction occurs?
A. Efficacy
B. Half-life
C. Concentration
D. Toxic potential
A. Efficacy
B. Half-life
C. Concentration
D. Toxic potential
Slide 53
Answer to Question #1
B. Half-life
Rationale: Along with affinity, the half-life (t12) of the inhibiting drug determines the duration of the interaction. The longer the half-life of the inhibiting drug, the longer the drug interaction lasts. Efficacy refers to the effectiveness of the drug. Concentration is a factor contributing to a drug's ability to inhibit hepatic enzymes. A threshold concentration must be reached or exceeded to inhibit an enzyme. Serious toxic potential may cause a drug to be removed from the market.
Rationale: Along with affinity, the half-life (t12) of the inhibiting drug determines the duration of the interaction. The longer the half-life of the inhibiting drug, the longer the drug interaction lasts. Efficacy refers to the effectiveness of the drug. Concentration is a factor contributing to a drug's ability to inhibit hepatic enzymes. A threshold concentration must be reached or exceeded to inhibit an enzyme. Serious toxic potential may cause a drug to be removed from the market.
Slide 54
Drug-Drug Interactions Caused by Induction
Result of the action of one drug (inducer) stimulating the metabolism of an object drug (substrate)
Enhanced metabolism produced by an increase in hepatic blood flow or an increase in the formation of hepatic enzymes
Increases the amount of enzymes available to metabolize drug molecules, thereby decreasing the concentration and pharmacodynamic effect of the object drug
Enhanced metabolism produced by an increase in hepatic blood flow or an increase in the formation of hepatic enzymes
Increases the amount of enzymes available to metabolize drug molecules, thereby decreasing the concentration and pharmacodynamic effect of the object drug
Slide 55
Excretion
Drugs are removed from the bloodstream by the kidneys by filtration or urinary secretion.
Reabsorption from the urine into the bloodstream may also occur.
Absorption may be affected by acidification or alkalinization of the urine and alteration of secretory or active transport pathways.
Although most drugs cross the membrane of the renal tubule by simple diffusion, some drugs are also secreted into the urine through active transport pathways.
Reabsorption from the urine into the bloodstream may also occur.
Absorption may be affected by acidification or alkalinization of the urine and alteration of secretory or active transport pathways.
Although most drugs cross the membrane of the renal tubule by simple diffusion, some drugs are also secreted into the urine through active transport pathways.
Slide 56
P-Glycoprotein Interactions
Inhibition or induction of P-glycoprotein (P-gp), an energy-dependent efflux transporter, can result in interactions involving absorption or excretion (biliary or renal).
P-gp pumps drug molecules out of cells and is found in the epithelial cells of the intestine (enterocytes), liver, and kidney.
P-gp pumps drug molecules out of cells and is found in the epithelial cells of the intestine (enterocytes), liver, and kidney.
Slide 57
Question #2
A practitioner prescribes a bicarbonate for a patient with severe heartburn. The practitioner knows that what factor caused by the drugs plays a key role in its excretion?
A. Enterohepatic recirculation
B. Alteration active transport pathways
C. Alkalinization of the urine
D. Induction of P-glycoprotein
A. Enterohepatic recirculation
B. Alteration active transport pathways
C. Alkalinization of the urine
D. Induction of P-glycoprotein
Slide 58
Answer to Question #2
C. Alkalinization of the urine
Rationale: Administration of bicarbonate can potentially increase the urine pH. This leads to the increased excretion of acidic drugs and the increased reabsorption of basic drugs.
Rationale: Administration of bicarbonate can potentially increase the urine pH. This leads to the increased excretion of acidic drugs and the increased reabsorption of basic drugs.
Slide 59
Pharmacodynamic Interactions
Pharmacodynamic profile: responses or effects produced by a drug's actions.
Drugs that have a similar characteristic in their pharmacodynamic profile may produce an exaggerated response.
Drugs may also produce opposing pharmacodynamic effects causing the expected drug response to be diminished or even abolished.
Drugs that have a similar characteristic in their pharmacodynamic profile may produce an exaggerated response.
Drugs may also produce opposing pharmacodynamic effects causing the expected drug response to be diminished or even abolished.
Slide 60
Drug-Food Interactions
Absorption: food can alter extent of drug absorption or change rate of drug absorption.
Metabolism: grapefruit juice inhibits the 3A4 subset of intestinal cytochrome P-450 enzymes and increases the serum concentration of drugs dependent on these enzymes for metabolism; food may also induce drug metabolism and therefore decrease drug efficacy.
Excretion: ingestion of certain fruit juices can alter the urinary pH and affect the elimination and reabsorption of drugs such as quinidine and amphetamine.
Metabolism: grapefruit juice inhibits the 3A4 subset of intestinal cytochrome P-450 enzymes and increases the serum concentration of drugs dependent on these enzymes for metabolism; food may also induce drug metabolism and therefore decrease drug efficacy.
Excretion: ingestion of certain fruit juices can alter the urinary pH and affect the elimination and reabsorption of drugs such as quinidine and amphetamine.
Slide 61
Effects of Food on Drug Pharmacodynamics
Food may oppose or potentiate pharmacologic action.
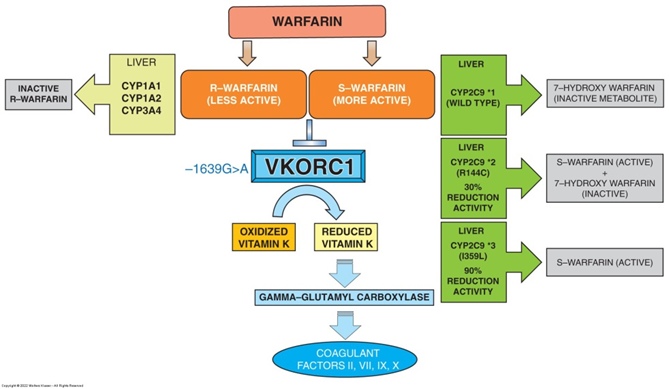
Warfarin reacts with foods containing vitamin K.
Monoamine oxidase (MAO) inhibitors can react with foods containing tyramine.
Some drugs can deplete nutrients or minerals found in foods.
Drug-induced malabsorption can occur in patients with preexisting poor nutritional status.
Drugs can change nutrient excretion.
Warfarin reacts with foods containing vitamin K.
Monoamine oxidase (MAO) inhibitors can react with foods containing tyramine.
Some drugs can deplete nutrients or minerals found in foods.
Drug-induced malabsorption can occur in patients with preexisting poor nutritional status.
Drugs can change nutrient excretion.
Slide 62
Question #3
A healthcare practitioner prescribes warfarin for a patient who Afib. The patient should avoid foods high in:
A. Potassium
B. Tyramine
C. Vitamin C
D. Vitamin K
A. Potassium
B. Tyramine
C. Vitamin C
D. Vitamin K
Slide 63
Answer to Question #3
D. Vitamin K
Rationale: Warfarin exerts its anticoagulant effects by inhibiting synthesis of vitamin K-dependent clotting factors. Vitamin K is required for activation by several protein factors of the clotting cascade, namely, factors II, VII, IX, and X. When foods rich in vitamin K are ingested, they can significantly oppose the anticoagulatory efficacy of warfarin.
Rationale: Warfarin exerts its anticoagulant effects by inhibiting synthesis of vitamin K-dependent clotting factors. Vitamin K is required for activation by several protein factors of the clotting cascade, namely, factors II, VII, IX, and X. When foods rich in vitamin K are ingested, they can significantly oppose the anticoagulatory efficacy of warfarin.
Slide 64
Complementary Alternative Medicine Interactions
Most herbal supplements are not regulated by the Food and Drug Administration (FDA).
Some herbs can prevent absorption of medications and reduce the effectiveness of those medications.
Acacia may impair the absorption of amoxicillin.
Dandelion may reduce effectiveness of quinolones.
Meadowsweet and black willow may displace highly protein-bound drugs.
Certain herbs can be inducers or inhibitors of the cytochrome P-450 enzyme system.
Some herbs can prevent absorption of medications and reduce the effectiveness of those medications.
Acacia may impair the absorption of amoxicillin.
Dandelion may reduce effectiveness of quinolones.
Meadowsweet and black willow may displace highly protein-bound drugs.
Certain herbs can be inducers or inhibitors of the cytochrome P-450 enzyme system.
Slide 65
Complementary Alternative Medicine Interactions #2
Some herbs may inhibit platelet activity and/or increase the INR.
Kava, lavender, and valerian may potentiate effects of central nervous system (CNS) depressants such as barbiturates and narcotics.
Kava may interfere with effects of dopamine or dopamine antagonists and is potentially hepatotoxic.
Aloe may cause hypoglycemia in patients taking glibenclamide.
Bitter orange may interfere with MAO inhibitor action.
Kava, lavender, and valerian may potentiate effects of central nervous system (CNS) depressants such as barbiturates and narcotics.
Kava may interfere with effects of dopamine or dopamine antagonists and is potentially hepatotoxic.
Aloe may cause hypoglycemia in patients taking glibenclamide.
Bitter orange may interfere with MAO inhibitor action.
Slide 66
Pharmacokinetic Interactions: Absorption
Absorption depends on the physiologic processes that maintain normal GI function.
Vitamin B12 deficiency is common in patients undergoing stomach surgery.
Diarrhea, a manifestation of many diseases, can pose a problem for oral absorption of drugs as well as food and nutrients.
Vitamin B12 deficiency is common in patients undergoing stomach surgery.
Diarrhea, a manifestation of many diseases, can pose a problem for oral absorption of drugs as well as food and nutrients.
Slide 67
Pharmacokinetic Interactions: Distribution
Conditions that may decrease plasma albumin levels:
Burns, bone fractures, acute infections, inflammatory disease, liver disease, malnutrition, and renal disease
Conditions that may increase plasma albumin levels:
Benign tumors, gynecologic disorders, myalgia, and surgical procedures
Burns, bone fractures, acute infections, inflammatory disease, liver disease, malnutrition, and renal disease
Conditions that may increase plasma albumin levels:
Benign tumors, gynecologic disorders, myalgia, and surgical procedures
Slide 68
Pharmacokinetic Interactions: Metabolism
Metabolism of drugs can be altered by disease that affect the functions of the liver (cirrhosis).
Heart failure is another disease that can cause direct reduction in ability of liver to metabolize drugs.
Use of a prodrug in patients with liver dysfunction can potentially reduce the efficacy of the drug.
Heart failure is another disease that can cause direct reduction in ability of liver to metabolize drugs.
Use of a prodrug in patients with liver dysfunction can potentially reduce the efficacy of the drug.
Slide 69
Effect of Diseases on Excretion of Drugs
Renal function can influence serum drug concentrations.
Glomerulonephritis, interstitial nephritis, long-term and uncontrolled diabetes, and hypertension are primary causes of declining renal function.
Drugs such as H2 receptor antagonists and fluoroquinolone antibiotics commonly require dose adjustments for patients with renal insufficiency.
Glomerulonephritis, interstitial nephritis, long-term and uncontrolled diabetes, and hypertension are primary causes of declining renal function.
Drugs such as H2 receptor antagonists and fluoroquinolone antibiotics commonly require dose adjustments for patients with renal insufficiency.
Slide 70
Effects of Drugs on Coexisting Disease
Drugs used to treat one medical condition can exacerbate the status of another comorbid disease.
This is particularly important in the elderly who have multiple concomitant diseases and often take multiple medications.
Detected rates of drug-disease interactions range from 6% to 30% in older adults.
This is particularly important in the elderly who have multiple concomitant diseases and often take multiple medications.
Detected rates of drug-disease interactions range from 6% to 30% in older adults.
Slide 71
Patient Factors Influencing Drug Interactions
Heredity
Disease
Environment
Smoking
Nutrition
Alcohol intake
Disease
Environment
Smoking
Nutrition
Alcohol intake
Slide 72
Adverse Drug Reactions
Definition: drug-induced toxic reactions
Two types of drug reactions
Type A reactions: exaggeration of the principal pharmacologic action of the drug
Type B reactions: unrelated to the principal pharmacologic action of the drug itself; precipitated by the secondary pharmacologic actions of the drug
Two types of drug reactions
Type A reactions: exaggeration of the principal pharmacologic action of the drug
Type B reactions: unrelated to the principal pharmacologic action of the drug itself; precipitated by the secondary pharmacologic actions of the drug
Slide 73
Tracking Drug Interactions and Adverse Drug Reactions
Causes of medication errors: look-alike and sound-alike drugs, dosage conversions, foreign drugs, illegible handwriting, unacceptable abbreviations
Tracking drug interactions and adverse drug reactions (ADRs)
The initial source of documented ADRs comes primarily from the experience gained while using a drug during clinical trials
MedWatch program: enhances the effectiveness of surveillance of drugs and medical products after they are marketed and as they are used in clinical practice
Tracking drug interactions and adverse drug reactions (ADRs)
The initial source of documented ADRs comes primarily from the experience gained while using a drug during clinical trials
MedWatch program: enhances the effectiveness of surveillance of drugs and medical products after they are marketed and as they are used in clinical practice
Slide 74
References
Arcangelo, V. (2022). Pharmacotherapeutics for Advanced Practice: A Practical Approach. 5th ed.
Wolters Kluwer. Philadelphia, PA
74
Wolters Kluwer. Philadelphia, PA
74