PPTX
Module 9 Insulin
Module 9: Endocrine, Diabetes, Insulin & Metabolic Disorders
Original source file is included in this package; the embedded viewer and full extracted text are available below.
Slide Text Extract
Improved reading view: slide text is enlarged, spaced out, and placed in expandable study cards. Use Expand all to read continuously, or search the whole textbook from the search box.
Images embedded in the deck are shown after the slide text. Open the original PPTX for exact slide layout.
Slide 1
Pharmacotherapeutics for Advanced Practice:
Insulin
N609
N609
Slide 2
Insulin
Rapid-acting: lispro (Humalog), aspart (NovoLog), or glulisine (Apidra), onset about 5 minutes, peaks in 1 hour, duration about 4 to 5 hours
Short-acting: "regular" (Humulin) insulin sometimes used around mealtime. Taken about 30 to 45 minutes before eating, peaks in 3 to 4 hours, duration 4 to 10 hours
Short-acting: "regular" (Humulin) insulin sometimes used around mealtime. Taken about 30 to 45 minutes before eating, peaks in 3 to 4 hours, duration 4 to 10 hours
Slide 3
Insulin
Intermediate-acting: NPH mixed with protamine, delaying absorption; insulin looks cloudy and has to be mixed before it is injected; onset one-half to 1 hour, peak 4 to 10 hours, duration 12 to 24 hours
Long-acting: glargine (Lantus),detemir (Levemir), degludec (Tresiba) insulins onset 2 to 4 hours, duration 24 hours with little or no peak
Long-acting: glargine (Lantus),detemir (Levemir), degludec (Tresiba) insulins onset 2 to 4 hours, duration 24 hours with little or no peak
Slide 4
Insulin
Pharmacokinetics
Absorption determined by type of insulin, injection site, and volume injected
Abdominal site absorbs 50% more than other sites
Metabolism: induces CYP1A2
Excretion: urine
Watch for standardized U 100/mL, needs U100 needles
ADRs: hypoglycemia, diabetic ketoacidosis
Watch alcohol use; increases hypoglycemia
Beta blockers mask hypoglycemia symptoms
Pregnant women can use rapid- or short-acting insulin; does not cross placenta
Insulin aspart, insulin glargine, and insulin glulisine
Absorption determined by type of insulin, injection site, and volume injected
Abdominal site absorbs 50% more than other sites
Metabolism: induces CYP1A2
Excretion: urine
Watch for standardized U 100/mL, needs U100 needles
ADRs: hypoglycemia, diabetic ketoacidosis
Watch alcohol use; increases hypoglycemia
Beta blockers mask hypoglycemia symptoms
Pregnant women can use rapid- or short-acting insulin; does not cross placenta
Insulin aspart, insulin glargine, and insulin glulisine
Slide 5
Insulin
Hypothyroidism: delays insulin breakdown; therefore may require less insulin units
Hyperthyroidism: increases renal clearance, requiring more insulin than baseline
Hyperthyroidism: increases renal clearance, requiring more insulin than baseline
Slide 6
Monitoring
Glycohemoglobin, renal function, CBC
A1C test twice a year in patients who are meeting treatment goals and have stable glycemic controls
A1C test quarterly in patients whose treatment has changed/not meeting goals
Point-of-care testing for A1C allows for timely decisions on treatments changes
A1C test twice a year in patients who are meeting treatment goals and have stable glycemic controls
A1C test quarterly in patients whose treatment has changed/not meeting goals
Point-of-care testing for A1C allows for timely decisions on treatments changes
Slide 7
Insulin: Patient Education
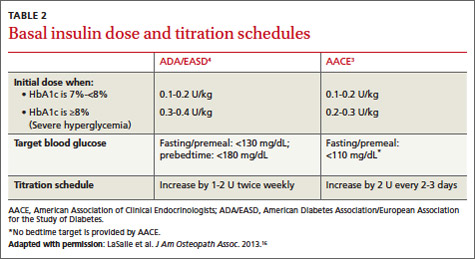
Goal A1C less than 7% for most nonpregnant adults
Individualized goals for older adults with long-time diagnoses
Administration, understanding types of insulin
Glucose monitoring frequency and recording
Emergency plan for glucose readings and "flu"
Lifestyle management, diet, exercise
Injection site selection
Individualized goals for older adults with long-time diagnoses
Administration, understanding types of insulin
Glucose monitoring frequency and recording
Emergency plan for glucose readings and "flu"
Lifestyle management, diet, exercise
Injection site selection
Slide 8
Insulin (continued)
Slide 9
Slide 10
Extracted Images / Illustrations